Professor Arjen Dondorp

Contact information
Podcast interview
The treatment of severe malaria
![]()
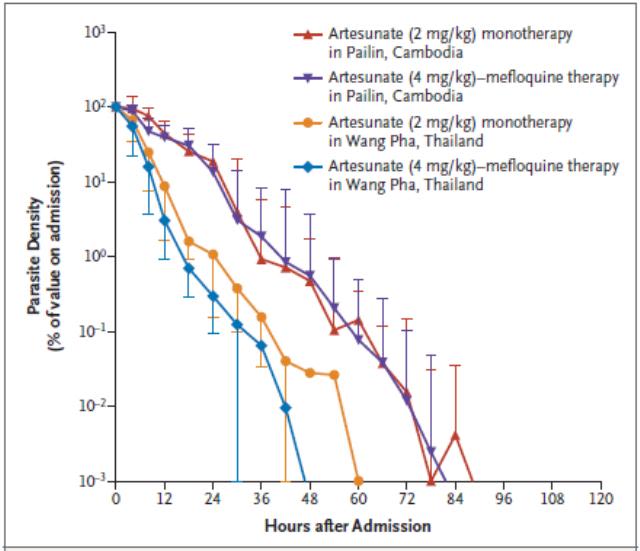
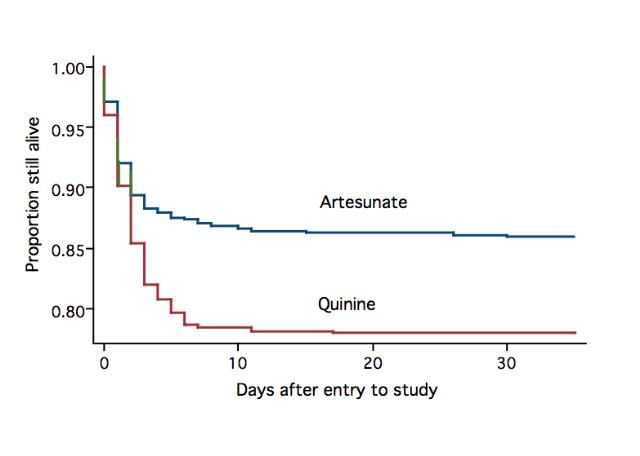
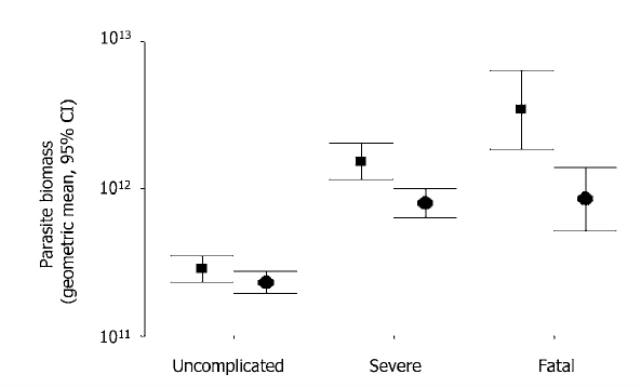
Successful malaria control has meant a drop in mortality rates worldwide but it is still an important disease. Therapies using artesunate, a derivative of artemisinin drugs, aim to kill malaria parasites before they mature. These therapies have high success rates and need to be developed. General care of malaria patients also needs to be improved.
Websites
-
Global Health in the New York Times, 19/11/18
Progress against malaria has stalled, and the disease remains a significant threat to billions of people despite the expensive, decades-long efforts to contain it. In an encouraging development, MORU reported complete success in curing hundreds of patients in Southeast Asia with new three-drug combinations mixing fast-acting artemisinin with two longer-lasting drugs. It it hoped that triple therapy should become the standard for malaria treatment.
Research groups
Arjen Dondorp
Professor of Tropical Medicine
- Deputy Director of the Mahidol Oxford Clinical Research Unit, Thailand
MORU
I am an intensive care and infectious diseases physician and trained in the Netherlands. Since 2001 I work at the Mahidol-Oxford Tropical Medicine Research Unit in Bangkok, Thailand where I am currently the Deputy Director and Head of the Malaria and Critical Illness Department. I am a Professor of Tropical Diseases at Oxford University, and a visiting Professor at the Mahidol University in Bangkok, Thailand.
My main research interests include the pathophysiology and treatment of severe malaria, antimalarial drug resistance, new treatments for drug resistant falciparum malaria and the improvement of intensive care practice in developing countries. In addition to my work at MORU, I currently chair the Regional Steering Committee for the Regional Artemisinin-resistance Initiative from the Global Fund. This is a large regional grant supporting the malaria elimination efforts in the Greater Mekong Subregion of Southeast Asia.
Recent publications
Severe Malaria A Research and Trials consortium - Multisite Adaptive Platform (SMAART MAP) Trial Protocol
Journal article
Maitland K. et al, (2026), Wellcome Open Research, 11, 414 - 414
Population Pharmacokinetics and Pharmacodynamics of Paracetamol in Malaysian Patients With Plasmodium knowlesi Malaria.
Journal article
Wattanakul T. et al, (2026), CPT: pharmacometrics & systems pharmacology, 15
Sevuparin in children with severe malaria: A phase I safety and dose finding trial
Preprint
Maitland K. et al, (2026)
Intravenous Artesunate in Artemisinin-Resistant Severe Malaria in Uganda
Journal article
Maitland K. et al, (2026), New England Journal of Medicine, 394, 2380 - 2382
Changing genetic profiles of Plasmodium falciparum piperaquine resistance in Southeast Asia over 25 years.
Journal article
Srisutham S. et al, (2026), Antimicrobial agents and chemotherapy, 70